A fractured shoulder can drastically limit how you use your arm, making everyday activities difficult and painful. This injury involves a break in one of the three bones that form the shoulder joint: the clavicle (collarbone), scapula (shoulder blade), or proximal humerus (the upper arm bone). These fractures often occur after a fall, accident, or direct blow to the shoulder, and may be accompanied by swelling, bruising, and difficulty moving the arm. Understanding what a fractured shoulder is, why it happens, and how it’s treated is an important step in navigating the recovery process.
Key Takeaways
- A fractured shoulder refers to a break in one of three bones (the clavicle, proximal humerus, or scapula).
- Many shoulder fractures, especially minimally displaced clavicle and proximal humerus fractures, heal well without surgery using a sling, rest, and guided rehabilitation.
- Surgery may be recommended when the fracture is significantly displaced, involves multiple fragments, or affects the shoulder joint surface.
The Anatomy of a Fractured Shoulder
The shoulder’s ball-and-socket structure allows for an incredible range of motion. This mobility, however, also makes it vulnerable to injury. A fractured shoulder involves a break in one or more of the three main bones that form the shoulder girdle.
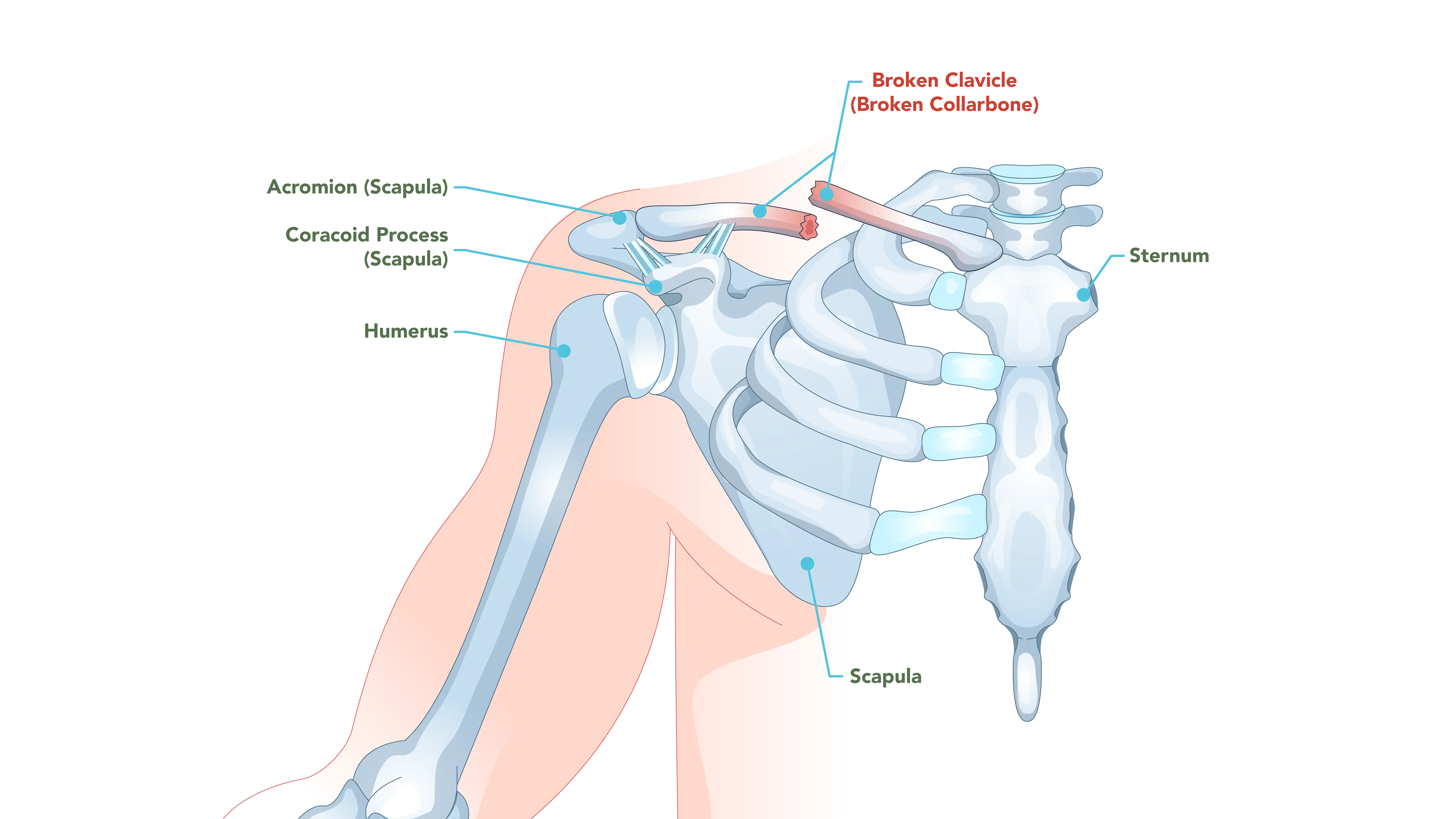
The Clavicle (Collarbone)
The clavicle is a long, slender bone connecting the sternum (breastbone) to the scapula (shoulder blade). It acts as a strut, keeping the shoulder positioned correctly away from the body. Clavicle fractures are common and are often seen in active individuals and children.
Many clavicle fractures result from a direct blow to the shoulder or, more frequently, a fall onto the point of the shoulder. A fall onto an outstretched hand can also transmit force up the arm, leading to a break. Common scenarios include bicycle accidents, contact sports injuries, and falls.
Treatment Considerations for Clavicle Fractures
The majority of clavicle fractures heal well without surgery. Non-operative treatment typically involves immobilizing the arm in a sling for comfort and support. Ice and oral pain medication may help manage the initial pain and swelling.
However, surgical intervention may be considered in specific cases. These might include fractures with significant displacement, meaning the broken bone fragments have shifted out of their normal alignment or no longer line up properly. The goal of surgical treatment is to restore the bone’s proper position and length, which can be particularly important for athletes or individuals with high physical demands.
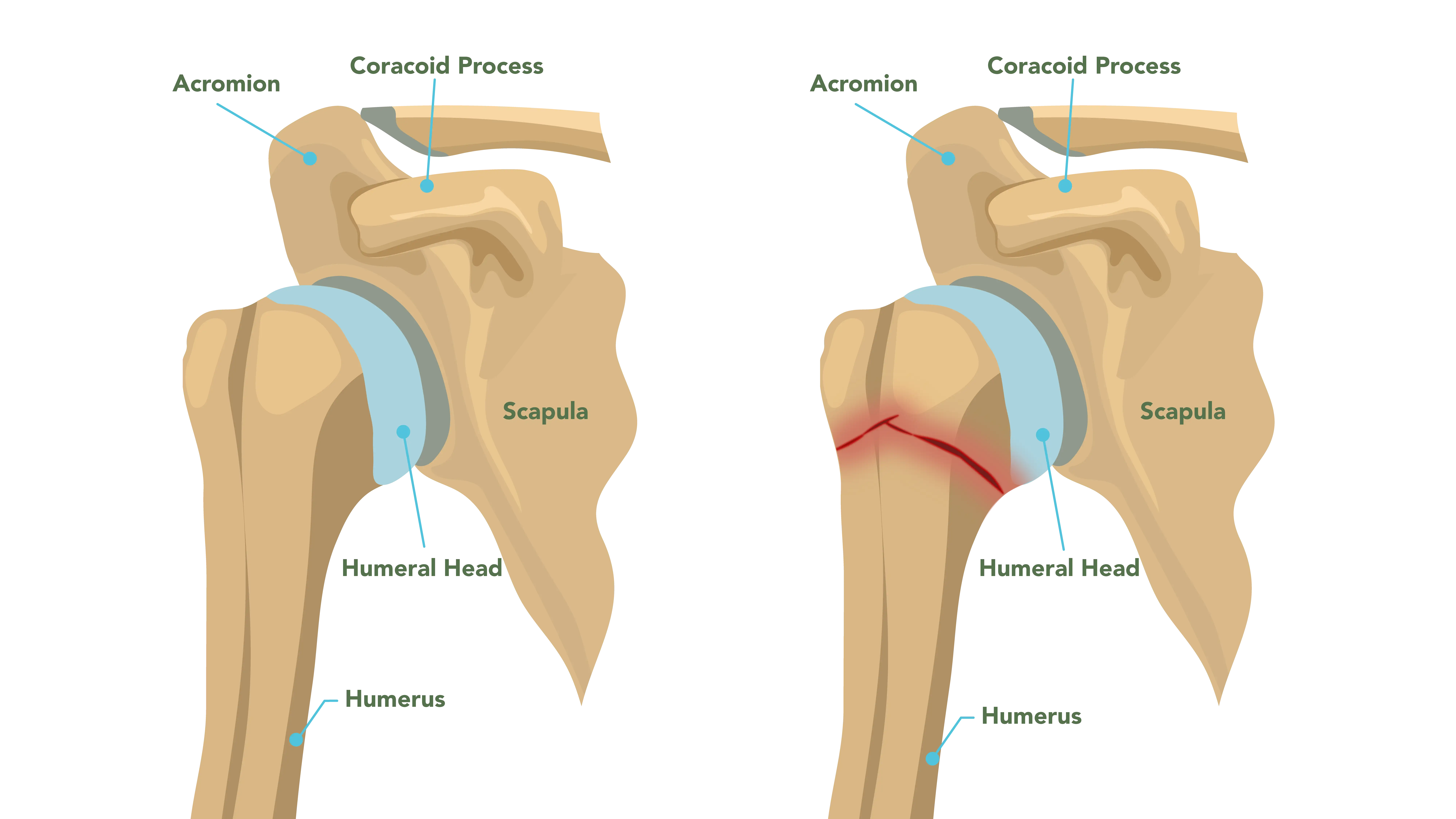
The Proximal Humerus (Upper Arm Bone)
The proximal humerus is the “ball” part of the shoulder’s ball-and-socket joint. Fractures here occur at the top of the humerus, close to the shoulder joint. These fractures can be especially common in older patients with osteoporosis, often resulting from a simple fall onto an outstretched hand or directly onto the shoulder. They can also occur in younger patients, but usually from high-energy trauma, such as a motor vehicle accident or a severe sports injury.
Classification and Complexity
Proximal humerus fractures are often classified using the Neer system, which categorizes the fracture based on the number of displaced “parts.” The proximal humerus is divided into four main regions: the humeral head, the greater tuberosity, the lesser tuberosity, and the shaft.
- Minimally Displaced (One-Part) Fractures: In these cases, the bone is broken, but the fragments remain in alignment.
- Two-Part, Three-Part, and Four-Part Fractures: These involve multiple fragments that are displaced or rotated. As the number of displaced parts increases, the fracture becomes more complex, and the likelihood of requiring surgery may increase.
Treatment Considerations for Proximal Humerus Fractures
For minimally displaced fractures, non-surgical treatment is the standard of care. This generally involves a period of immobilization in a sling, followed by a structured physical therapy program. Surgical options may be recommended when the fracture is severely displaced, involves the joint surface, or is a complex fracture.
The Scapula (Shoulder Blade)
Scapula fractures are relatively rare. The shoulder blade is a broad, flat bone, well-protected by a thick layer of muscle and the rib cage. Because of this protection, a scapula fracture usually indicates a high-energy trauma, such as a major car accident or a significant fall. These injuries also frequently involve chest trauma.
Causes and Risk Factors for a Fractured Shoulder
A fractured shoulder can happen to anyone, but certain activities and underlying health conditions may increase the risk. Understanding these factors can aid in prevention.
For younger, healthy individuals, a shoulder fracture is frequently the result of a high-energy event, including motor vehicle accidents, falls from a height, or contact sports.
In older adults, particularly those over the age of 65, a common cause of a fractured shoulder is a fall from a standing height. This is largely due to osteoporosis, a condition that causes bones to become weak and brittle. Additionally, age-related changes in balance and muscle strength may increase the frequency of falls, which in turn increases the risk of fracture.
Recognizing the Signs and Symptoms
If you suspect a fractured shoulder, recognizing the signs quickly is helpful for seeking prompt medical attention. While symptoms can vary depending on the bone involved and the severity of the break, several common indicators are generally present:
- Severe Pain: The pain is usually immediate and intense at the time of injury. It frequently worsens with any attempt to move the arm or shoulder.
- Swelling and Bruising: Swelling around the shoulder joint and the upper arm is typical. Bruising may appear quickly or develop over the next few days.
- Inability to Move the Arm: The patient may be unable to lift the arm away from the body or move it. They often instinctively support the injured arm with the uninjured one.
- Deformity or Bony Prominence: In some displaced fractures, a visible bump, lump, or abnormal contour may be present, particularly with clavicle fractures.
- Grinding Sensation (Crepitus): A grating or popping sensation may be felt or heard when attempting to move the shoulder.
Diagnosis and Initial Management
The diagnostic process for a fractured shoulder is typically straightforward, beginning with a physical examination and imaging studies.
- Physical Examination: Your doctor will carefully assess the injury, looking for swelling, bruising, and any obvious deformity. They may also check the patient’s neurological and vascular status by testing sensation and circulation in the arm and hand.
- X-rays: Standard X-rays are the primary tool for diagnosing a shoulder fracture. They can provide images of the bone structure, confirming the presence of a break, its location, and the degree of displacement. Multiple views are usually taken to fully visualize the fracture pattern.
- Other Imaging: For more complex fractures, especially those involving the joint surface (glenoid or complex proximal humerus fractures), a CT scan may be recommended. If your doctor suspects soft tissue damage, magnetic resonance imaging (MRI) may be used.
Treatment Pathways: Non-Surgical vs. Surgical
The decision to treat a fractured shoulder non-surgically or surgically is highly individualized, depending on the patient’s age, activity level, bone quality, and the specific characteristics of the fracture. An experienced shoulder specialist can evaluate the injury and guide the most appropriate treatment path.
Non-Surgical Management
Non-operative treatment is the preferred approach for many shoulder fractures, particularly those that are minimally displaced or stable. Oral medications and ice may be recommended for pain management during healing.
- Immobilization Phase: The arm remains in a sling for a set period for initial healing. During this time, the patient is often instructed to perform gentle, passive range-of-motion exercises for the elbow, wrist, and hand to prevent stiffness.
- Early Motion Phase: Once your doctor determines the fracture is stable, a physical therapy program begins. This phase focuses on restoring passive range of motion.
- Strengthening Phase: As healing progresses, the focus may shift to active range of motion and strengthening exercises. The goal is to rebuild muscle strength lost during immobilization and restore full function.
Surgical Management
Surgery may be recommended when the fracture is unstable, displaced, or involves the joint surface in a way that would compromise long-term function.
Surgical options may include Open Reduction and Internal Fixation (ORIF), where the surgeon realigns the bone fragments and secures them with metal hardware (plates, screws, or pins). This is common for displaced clavicle and complex proximal humerus fractures. Intramedullary nailing may be used for some humerus fractures, involving a rod inserted down the center of the bone.
For complex proximal humerus fractures or those with compromised blood supply, shoulder replacement surgery may be recommended, with the reverse option often preferred for older patients with complex fractures and pre-existing rotator cuff issues.
Following surgery, the arm is immobilized in a sling for a period of time. The rehabilitation protocol is similar to non-surgical treatment but is carefully timed to protect the surgical repair. The surgeon and physical therapist work closely to ensure motion is regained without jeopardizing the hardware or the healing bone.
Summary
A fractured shoulder is a significant injury, but with the right diagnosis, treatment plan, and rehabilitation, many patients experience improvement in pain, motion, and function over time. Whether the fracture involves the clavicle, proximal humerus, or scapula, understanding the type of break and how it affects the shoulder joint is key to guiding treatment. Many fractures heal well with non-surgical care such as sling immobilization, rest, and physical therapy, while others, particularly those that are displaced or involve the joint surface, may benefit from surgical stabilization.
Frequently Asked Questions
How long will I need to wear a sling for a fractured shoulder?
The duration of sling use varies significantly based on the type and severity of the fracture. It is important to follow your doctor’s specific instructions, as removing the sling too early may disrupt the healing process.
Will I need physical therapy after a shoulder fracture?
In most cases, yes. Even if the fracture heals perfectly, the shoulder joint can become stiff after a period of immobilization. Therapy helps to safely restore the range of motion and rebuild the strength in the surrounding muscles.
What is the difference between a shoulder fracture and a shoulder separation?
A fractured shoulder involves a break in one of the bones (clavicle, humerus, or scapula). A shoulder separation, on the other hand, is an injury to the ligaments that connect the clavicle to the scapula at the acromioclavicular (AC) joint. While both are shoulder injuries and can occur from similar trauma, they involve different structures.
