Shoulder Disorders Palm Beach County
(561) 746-7686
1002 S Old Dixie Hwy Jupiter, FL 33458
Monday - Thursday | 8:00 AM - 5:00 PM
Friday | 8:00 AM - 3:00 PM
Specialties

Discover Recent Posts

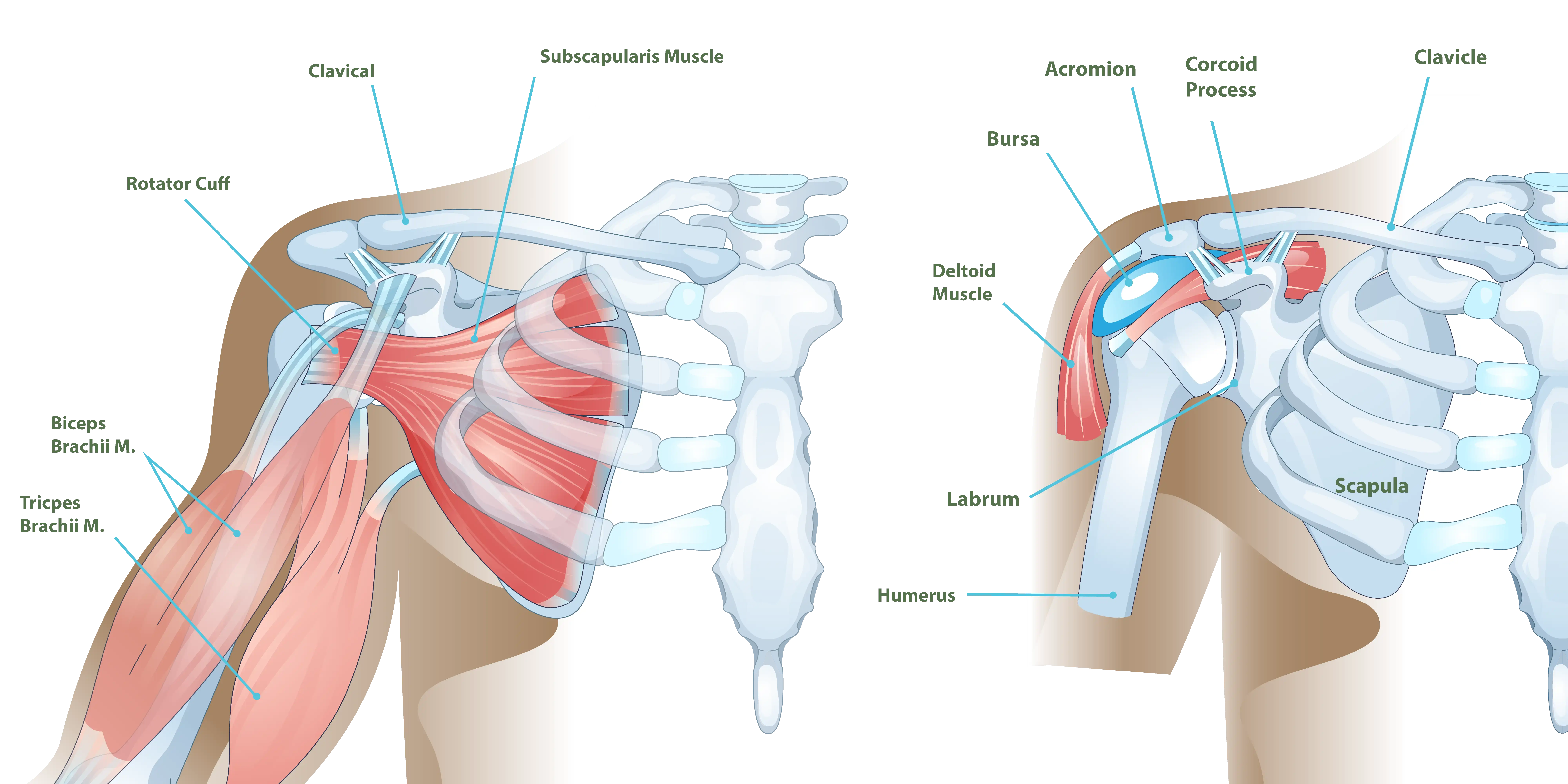
Shoulder Anatomy
The shoulder consists of three primary bones: the collarbone (clavicle), the shoulder blade (scapula), and the upper arm bone (humerus). Its main role is to help position the arm and hand in space. While it is commonly called a ball-and-socket joint, it actually functions more like a golf ball resting on a tee, supported by muscles and tendons known as the rotator cuff.
Because of this structure, the shoulder is the most mobile joint in the human body. It allows for a wide range of movements, including reaching overhead, behind the back, across the body, and out to the side. This range of motion is what makes it possible to throw a ball, swing a golf club or tennis racket, get dressed, or grab something from a high shelf.
Although the shoulder’s unique structure allows for a wide range of movement, it is also more prone to problems such as instability, soft tissue damage, and fractures.
Dr. Diaz focuses on delivering focused care for shoulder conditions. During your consultation, she will work to identify the source of your symptoms or limitations. The visit will also involve creating a personalized treatment plan that takes into account your activity level and goals, the state of your shoulder, and your overall health.
Specific Shoulder Conditions
Rotator Cuff Tears
Rotator cuff conditions affect millions of individuals and are a leading cause of shoulder pain and dysfunction. The rotator cuff plays a key role in both stabilizing the shoulder and enabling its movement. It consists of four muscle tendon units that surround the shoulder joint.
Rotator cuff issues exist on a spectrum. These can range from partial and full-thickness tears that can be surgically repaired, to large, chronic tears that may no longer be repairable. Common signs and symptoms of a rotator cuff tear include:
- Shoulder pain that disrupts sleep
- Difficulty taking part in sports or exercise
- Pain or challenges while getting dressed (such as putting on a belt or shirt)
- Pain and/or weakness when trying to raise the arm
- Inability to lift the arm
- Discomfort or reduced strength when lifting or carrying objects
- Pain or difficulty when grooming, such as styling hair, shaving, or applying makeup
- Difficulty with tasks like steering, closing a car door, or reaching for a seatbelt
Some rotator cuff tears occur after a specific traumatic injury, but most develop gradually through wear and tear over time. As individuals age, they become more likely to experience problems with their rotator cuff. Over a five year period, tears that initially caused no symptoms may eventually lead to pain or reduced function.
Rotator cuff tears are common. This high rate of occurrence is due to several factors. One significant reason is that the blood flow to rotator cuff tendons decreases with age, which limits the tendons’ ability to recover from routine stresses. Additionally, some individuals have bone shapes that make them more prone to developing these tears.
Dr. Diaz treats hundreds of patients each year with rotator cuff tears and helps them experience reduced pain and better shoulder mobility through arthroscopic rotator cuff repair. This procedure involves reattaching the torn tendon to the bone using small incisions around the shoulder. With specialized tools, Dr. Diaz places anchors in the bone and secures the tendon back into position.
Surgery is not always necessary for rotator cuff tears. Depending on the specific case, many people can achieve meaningful relief and improved function with a nonoperative approach that includes physical therapy, modifying certain activities, and regular follow ups with Dr. Diaz to monitor the condition and address any changes.
Rotator Cuff Tear Arthritis
The shoulder joint relies on muscles and tendons for stability rather than bone, which gives it remarkable flexibility and allows us to move our hand freely through space. However, this high degree of mobility comes at a cost, as its stability depends on the health and function of the four key muscle tendon units that make up the rotator cuff: the supraspinatus, infraspinatus, teres minor, and subscapularis.
Many individuals with a painful rotator cuff tear can be effectively treated using arthroscopic techniques. In contrast, large chronic tears may no longer be repairable and can lead to cuff tear arthritis. In these cases, the damaged muscles can no longer hold the humerus properly centered in the socket, causing the arm bone to shift upward and out of alignment.
This loss of joint control limits the ability to move the hand into certain positions, making everyday tasks like reaching overhead, getting dressed, participating in sports, turning a steering wheel, or eating more difficult. Cuff tear arthritis is typically marked by intense pain and restricted motion. For many patients, reverse shoulder replacement offers reliable relief and improved function.
Osteoarthritis
Osteoarthritis, also known as degenerative arthritis, is the most common type of arthritis and affects millions across the United States. It occurs when the cartilage that cushions the joint gradually breaks down due to wear and tear. Several factors contribute to its development, including age, genetic predisposition, activity level, type of work, and other underlying health conditions.
As the cartilage deteriorates, inflammation develops within the joint, often leading to significant pain, reduced mobility and strength, and difficulty sleeping. When non-surgical approaches such as medications, physical therapy, and adjustments in diet and lifestyle no longer offer adequate relief, Dr. Diaz may recommend a total shoulder replacement as the next step in treatment.
AC Arthritis
The acromioclavicular (AC) joint is where the end of the collarbone (clavicle) meets a part of the shoulder blade known as the acromion, which forms the bony roof of the shoulder. Although this joint is small, it undergoes significant stress during activities that involve forceful movements above eye level, which can lead to early cartilage wear. When the cartilage within the AC joint breaks down, acromioclavicular arthritis can develop. Individuals such as manual laborers and weightlifters are especially prone to experiencing symptoms related to this condition.
AC joint arthritis typically causes pain and swelling at the top of the shoulder. Symptoms often come and go but are most noticeable during overhead activities (like a military press), reaching across the body, or lying on the affected side during sleep.
When nonoperative treatments such as rest, physical therapy, and medication are no longer effective, surgery may be considered. The surgical approach usually involves removing a small section from the end of the clavicle to prevent bone-on-bone contact, which is the source of pain.
Dr. Diaz typically performs this procedure arthroscopically, which offers benefits such as faster recovery, lower risk of joint instability, and no external incision over the top of the shoulder (avoiding an area that can be sensitive to contact from clothing or bag straps). Most patients are able to return to their normal level of activity, including sports, within six weeks. However, if this procedure is done alongside a reconstructive surgery, such as a rotator cuff or labral repair, the recovery plan and restrictions will depend on that accompanying procedure.
AC Separation
A hard impact to the tip of the shoulder can cause a separation of the acromioclavicular (AC) joint. This type of injury is especially common among cyclists and football players. In many cases, the injury can heal without surgery, and individuals often regain full, pain-free shoulder function, even if some visible deformity remains.
However, when the separation is more severe and the joint is significantly out of place, an arthroscopically assisted procedure to reconstruct the supporting ligaments of the AC joint may be recommended.
Biceps Tears and Tendinitis
One of the tendons of the biceps begins inside the shoulder joint, running between two of the rotator cuff tendons before continuing down the front of the arm to join the main part of the biceps muscle. This portion, known as the long head of the biceps, is a common source of shoulder pain. Tears can result from injury or overuse. While many biceps tears can be treated non-surgically, depending on the extent of the tear, surgical arthroscopy may be performed to repair the tear when necessary.
Clavicle Fractures
The collarbone acts as a support beam for the arm and plays a key role in maintaining proper shoulder function. Many clavicle fractures can be managed without surgery by using a sling to keep the shoulder still while the bone heals. Applying ice and taking oral pain relievers can help reduce discomfort during this period.
In cases where the broken ends of the bone are significantly displaced or overlapping, surgery may be recommended. Surgical treatment typically involves using a plate and screws or an internal device to realign the bone, promote healing, and protect shoulder function.
If your treatment plan involves wearing a sling and avoiding shoulder movement, you are still encouraged to remove the sling periodically to move your elbow and fingers. These motions help with daily tasks like eating, brushing your teeth, or performing light activities such as typing or writing at a table.
Once imaging confirms that the bone is healing properly, you can begin moving your shoulder to position your hand for everyday tasks. Heavier activity, such as doing chores, yard work, or playing sports, should be postponed until advised that it is safe to resume.
Frozen Shoulder
Frozen shoulder, medically referred to as adhesive capsulitis, occurs when the soft tissue lining of the shoulder joint (the capsule) goes through a process of inflammation, thickening, and scarring. This condition is most frequently seen in individuals between the ages of 40 and 65, with women affected more often than men. While some cases are linked to a previous shoulder injury or surgery, many arise without a clear cause. Known risk factors include diabetes and thyroid disorders.
People with frozen shoulder often report the onset of shoulder pain without a significant injury, or following what seems like a minor one. Discomfort during the night is common, and many experience difficulty performing daily activities such as brushing their hair or getting dressed. As the condition progresses, stiffness sets in, limiting range of motion.
Over time, the pain gradually subsides and the shoulder begins to regain mobility. This is a phase sometimes referred to as “thawing.” Reaching this stage typically requires consistent stretching, managing any underlying thyroid issues or diabetes, and maintaining patience throughout the process.
Most individuals recover without the need for surgery. Symptom relief may come from physical therapy, oral anti-inflammatory medications, and corticosteroid injections. Some patients also find benefit in acupuncture, meditation, or biofeedback techniques. Dietary changes, such as adopting a low-inflammation diet high in fiber and avoiding sugary, processed foods, can also support recovery.
Frozen shoulder usually resolves within 12 to 18 months, although the timeline can vary. In people with diabetes, the course of frozen shoulder tends to be longer and recurrences are more common. Cases triggered by trauma often require more aggressive therapy and may not resolve naturally without intervention.
Proximal Humerus Fractures
Fractures of the upper arm bone, or proximal humerus, are relatively common. Pain can usually be managed with ice, a sling for support, and oral pain relievers. While most of these fractures can heal without surgery, certain cases may require surgical intervention or even shoulder replacement to restore proper function and alignment.
While proximal humerus fractures often occur in older adults with decreased bone density, typically after a fall, fractures are not limited to older individuals. They can also affect younger patients who experience high-impact trauma, such as from motor vehicle accidents or sports injuries. Initial treatment usually involves immobilizing the shoulder with a sling.
Whether to proceed with surgery depends on factors such as the position and type of fracture, the presence of a dislocation, and the patient’s activity level and overall goals. It’s important to note that these injuries can sometimes involve damage to the nerves that control arm movement and sensation.
If your treatment includes a period of immobilization with a sling, plan to still regularly move your fingers and bend and straighten your elbow to maintain function for daily activities like eating and brushing your teeth. However, more strenuous activities including sports, housework, and yard work should be avoided until confirmed it is safe to resume them.
Shoulder Instability and Labral Injuries
A labral tear occurs when the ring of cartilage that lines the edge of the shoulder socket, called the glenoid, becomes damaged. This tissue acts as a stabilizer by keeping the ball of the upper arm bone centered in the socket.
Labral injuries can result from traumatic events like a dislocated shoulder or from repetitive stress. Initial management usually involves rest, avoiding aggravating movements, and strengthening exercises for the shoulder. If symptoms do not improve with conservative care, surgery may be considered.
Athletes who perform repeated overhead motions, as well as other active individuals, can develop painful injuries to the upper portion of the labrum. These injuries are known as SLAP tears, short for superior labrum anterior to posterior. This type of tear involves the area where the biceps tendon attaches to the labrum.
Many SLAP tears do not require surgery and are managed with physical therapy. However, for some individuals who sustain SLAP tears from trauma, surgical repair might be needed to restore shoulder function and stability.
When nonsurgical treatment fails, minimally invasive arthroscopic procedures can be performed. These may include trimming damaged tissue or repairing the labrum, and in some cases, addressing the biceps tendon with either a tenotomy (releasing the tendon to allow healing through scar formation) or a tenodesis (reattaching the tendon to the upper arm with an implant).
Younger patients who experience a shoulder dislocation or instability may develop a Bankart lesion, which is a tear in the lower front portion of the labrum. Those who plan to return to high-risk sports or activities that involve forceful shoulder movements, such as football, wrestling, surfing, or wakeboarding, may need surgery if physical therapy does not lead to improvement.
Surgical stabilization is more commonly recommended in young or highly active patients with Bankart tears who are at increased risk for recurrent dislocations. First-time dislocations are sometimes treated with rest and therapy aimed at strengthening the shoulder muscles that help maintain joint stability. Surgeons take several factors into account when deciding between surgery and continued nonoperative care:
Age: Younger patients, especially those under 20, are at a higher risk of dislocating again without surgical repair.
Activity level: Those involved in contact sports or activities with a high chance of reinjury may benefit more from early surgery.
Joint flexibility: People with naturally loose joints or hypermobility have an increased chance of recurrent instability.
Bone damage: Repeated dislocations can cause injury to the bone of the ball or socket, making surgical repair more appropriate.
Recovery times vary depending on the injury and selected treatment plan. The goal of both nonsurgical and surgical treatment is to relieve pain and restore function to the shoulder.
Subacromial Impingement (Bursitis)
The bony ceiling of the shoulder is a part of the shoulder blade or scapula called the acromion. There is wide variability in the shape of the acromion from one person to the next. Certain people are predisposed to inflammation in the space below the acromion (subacromial space) and above the rotator cuff.
This inflammation often manifests as pain halfway down the arm that is provoked by reaching behind one’s back or above the head. Occupational or recreational pursuits that involve sustained eye-level or above motions can increase the risk of this condition, called impingement or bursitis.
If the acromion is prominent towards the front or side of the shoulder, this may predispose to impingement. Poor posture from muscle imbalance or from curvature of the spine as we age and lose bone mass can also increase the risk of this and other shoulder conditions.
Most cases of subacromial impingement can be managed with a high quality physical therapy or physician-directed home exercise program. Some patients may benefit from a local injection to calm down the pain and inflammation.
Other patients may benefit from an arthroscopic procedure to remove inflamed tissue and smooth out the undersurface of the bony prominence. This is especially true if there is a co-existing rotator cuff tear.
Treatment & Recovery
Shoulder care is most effective when tailored to each patient’s unique needs and lifestyle. Dr. Diaz offers a thorough, patient-centered approach to guide individuals through every stage of treatment and recovery.
- Non-Surgical Treatments: Physical therapy focused on strengthening and stabilizing the shoulder, activity modification, anti-inflammatory medications, and injections to reduce pain and inflammation.
- Surgical Treatments: Arthroscopic procedures for repairs and stabilization, total or reverse shoulder replacements to restore function. In some cases, advanced techniques like tenodesis or tenotomy may be recommended.
- Rehabilitation and Prevention: Customized rehabilitation programs to restore strength, improve range of motion, and reduce the risk of future injury. Patients also receive education on safe movement patterns and conditioning strategies to protect the shoulder long term.
Shoulder pain and instability don’t have to limit your life. With expert care from Dr. Diaz, patients throughout the region regain function, reduce pain, and return confidently to their favorite activities through personalized treatment and comprehensive rehabilitation.